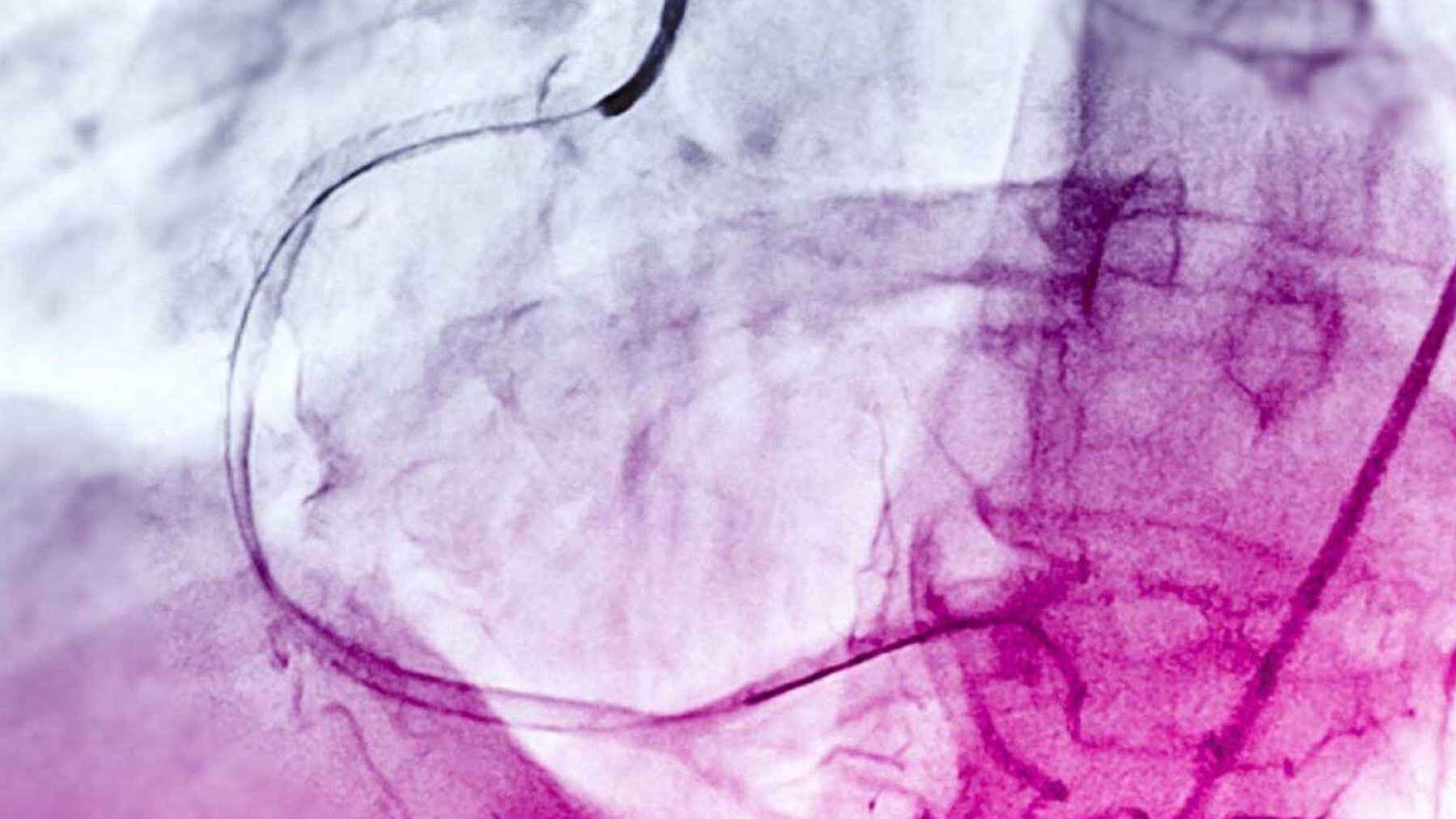
During a coronary angiogram, doctors watch blood move through the heart’s arteries on a live X-ray screen. The view can be messy. Vessels are thin, the image may shake, and bones, stents, or surgical grafts can sit in the background like visual clutter.
A new preprint led by Elakiya Sivakumar at Columbia University reports a targeted fix for that problem. By fine-tuning MedSAM2 for coronary angiograms, the system improved from roughly 3 out of 100 to roughly 77 out of 100 on a vessel-overlap score in 200 validation images, then tracked arteries consistently in most test videos. The point is not that AI suddenly became a cardiologist. It is that a broad vision model needed careful medical training before it could follow the right lines.
Why tracing arteries is hard
Segmentation means outlining the part of an image that matters. In this case, that part is the coronary artery tree, the branching network that feeds the heart muscle and can narrow during coronary artery disease.
That sounds simple until you see fluoroscopy, which is live X-ray video. Contrast dye helps the vessels show up, but the picture is still flat, noisy, and often crowded. It can feel a bit like tracing a thin river through fog while the fog keeps moving.
The ARCADE challenge was created for this exact bottleneck. Its organizers note that manually selecting coronary segments and stenotic lesions is costly and time-consuming, which is why automated tools are being tested for angiography analysis.
What the AI is built from
The new work starts with Meta’s Segment Anything Model 2, usually called SAM2. Meta describes it as a unified model that can select objects in images and videos using prompts such as a click, a box, or a mask, and then keep track of that object across frames.
For medicine, the study used MedSAM2, a version adapted for medical images and video. Jun Ma, Bo Wang, and collaborators built that system with several institutions, including University Health Network, the Vector Institute, Harvard Medical School, and the University of Toronto. They utilized large sets of medical images and video frames for development.
Fine-tuning is the key move here. Instead of asking the model to solve a new hospital task cold, Sivakumar trained it on coronary angiograms so it could learn the look of faint vessels, dye-filled branches, and distracting hardware.
The training set
The model was trained and tested with the ARCADE coronary angiography data. The public Phase 1 set includes 1,200 vessel-tree images, split into 1,000 training images and 200 validation images, with annotations showing where the coronary vessels are.
The GitHub record for the project says the team used a single click near the center of the target vessel as a prompt. It also reports that training expanded the examples through rotations and flips, a common way to help software deal with different viewing angles without collecting a brand-new hospital archive.
The score jumped
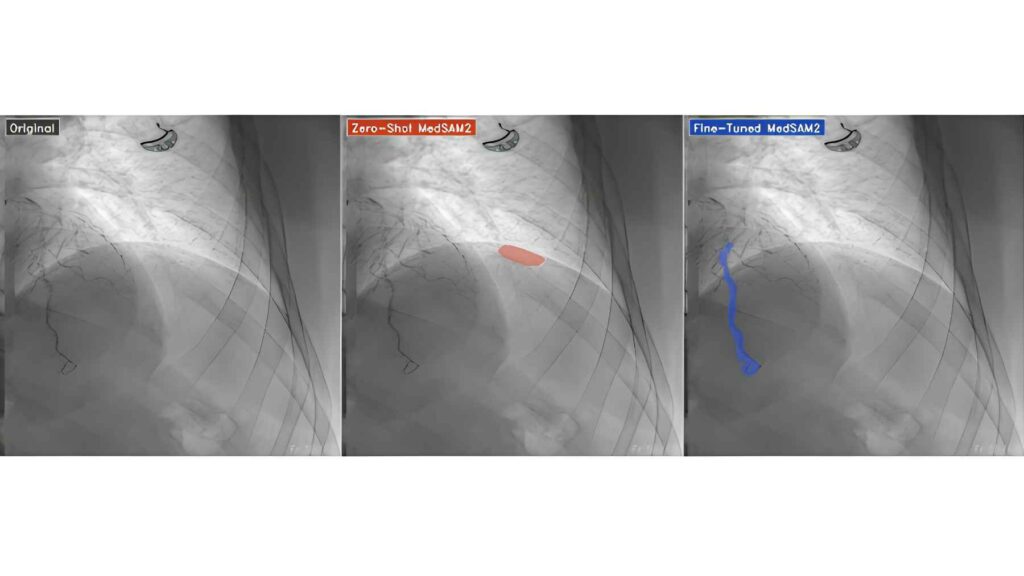
The main result is easy to grasp. Before training on this task, the model’s Dice score was about 3 out of 100. After fine-tuning, it rose to about 77 out of 100 on the same validation set.
A Dice score is an overlap score. If the AI outline and the human outline sit on top of each other, the score gets closer to 100. If they barely match, the score stays low.
What does that mean in a hospital? Not an automatic diagnosis. It means the software became much better at drawing the artery, which is a possible building block for measuring vessel shape, spotting changes, or reducing tedious manual tracing.
Video was the real test
Still images are only one part of the story. Coronary angiography is a moving exam, and the new model was also applied to 10 fluoroscopy studies from the CoronaryDominance video dataset.
In 9 of those 10 studies, the fine-tuned model followed vessels coherently and avoided wrongly highlighting ribs, stents, and bypass grafts, according to the study summary. That matters because a false outline can pull attention away from the structure the doctor actually needs to see.
The video result comes with a catch. The project describes it as a qualitative test because there were no frame-by-frame human labels for every video. In other words, the model looked promising, but the video evidence is not yet the same as a full scored benchmark.
Why this could matter
In practical terms, better artery segmentation could make image analysis faster at the point of care. During a procedure, every extra step competes with the patient, the screen, the catheter, and the clock.
At the end of the day, the useful tool is not the flashiest AI model. It is the one that quietly marks the right vessel and stays out of the way. No cardiologist wants software that mistakes a rib for an artery during a critical moment.
Experts will still need broader testing. The system should be checked across hospitals, scanner brands, image quality levels, patient groups, and real clinical workflows before anyone treats it as a dependable medical assistant.
Open tools, early caution
The project’s code is available on GitHub, and the fine-tuned checkpoint is listed on Hugging Face. That makes the work easier for other researchers to inspect, repeat, or challenge, which is especially important in medical AI.
There is also a big caution sign. medRxiv says its manuscripts are posted before peer review, so the findings should be treated as preliminary and should not guide clinical care on their own.
Even with that caution, the study points to a clear lesson. General AI vision tools can be powerful starting points, but the heart is not a vacation video or a street scene. For medical images, the details matter.
The official preprint has been published on medRxiv.